
Patient groups have been expanded to 6 categories and it is worth pointing out that the neonate, infant and paediatric weight of has now wider range and on contrary the adult weight has lower limit of 56 kg as opposed to 70kg.
| Patient group according to ISO 18562-1 2017 | Patient group according to ISO 18562-1 2024 | ||
| Neonate | 0,5 kg | Premature neonate | <2,65 kg |
| Infant | 3,5 kg | Infant 0- 0.5 yr | 2,65-7,4 kg |
| Small child 0,5-3yr | 7,4-15 kg | ||
| Paediatric | 10kg | Child 3-10yr | 15-32 kg |
| Adolescent 10-18yr | 32-56 kg | ||
| Adult | 70kg | Adult >18yr | >56 kg |
On this note, new terms and guidance on resting breath rate, and default daily breathing volume when resting have been introduced. These new values and definitions will have an impact in the further testing to be performed, if deemed necessary such as to estimate the inhalation dose to the patient for the tests of ISO 18562-3, convert the concentration of each substance to a total dose per patient per day based on the breathed volume.
| Patient group | Label | Typical age range | Ideal body mass range (kg) | LPV (ml/kg) | Resting breath rate (breaths/min) | Default body mass (kg) | Default daily breathing volume (resting) (m3/d) | Maximum exercise ventilation (m3/h) |
|---|---|---|---|---|---|---|---|---|
| Premature | neonate | Premature birth | <2.65 | 6 | 60 | 0.5 | 0.26 | — |
| Infant | 0 to 0.5 | 2.65 to 7.4 | 8 | 56 | 44 | 3.5 | 2.3 | — |
| Small child | 0.5 to 3 | 7.4 to 15 | 8 | 44 | 26 | 5.1 | 6.0 | 1.8 |
| Child | 3 to 10 | 15 to 32 | 8 | 26 | 20 | 20 | 7.7 | 2.6 |
| Adolescent | 10 to 18 | 32 to 56 | 8 | 21 | 32 | 7.7 | 11.5 | 4.6 |
| Adult | >18 | >56 | 8 | 20 | 60 | 11.5 | 4.6 | — |
Single transitory contact duration with accumulative limited exposure has now been included into the consideration and with their evaluation can be completed with good rationale. For example: Single use inhalers, respiratory gas monitors, mouth pieces and masks would not require testing with the justification given, however thorough review of the coatings applied to those will have to be evaluated.
The new important Annex ZA has been added, where the relationship between International standard and European Standard edition as a presumption of conformity has been established.
The risk management process has changed to more detailed version which supports the risk management process not only with detailed aspects and conditions of the studies. It also includes the weight of the rationale in this process which allows to avoid unnecessary tests that would provide no value to the risk evaluation.
It is also now clearly stated that the same risk evaluation standard will be used throughout the ISO 18562 the same as used within ISO 10993 series.
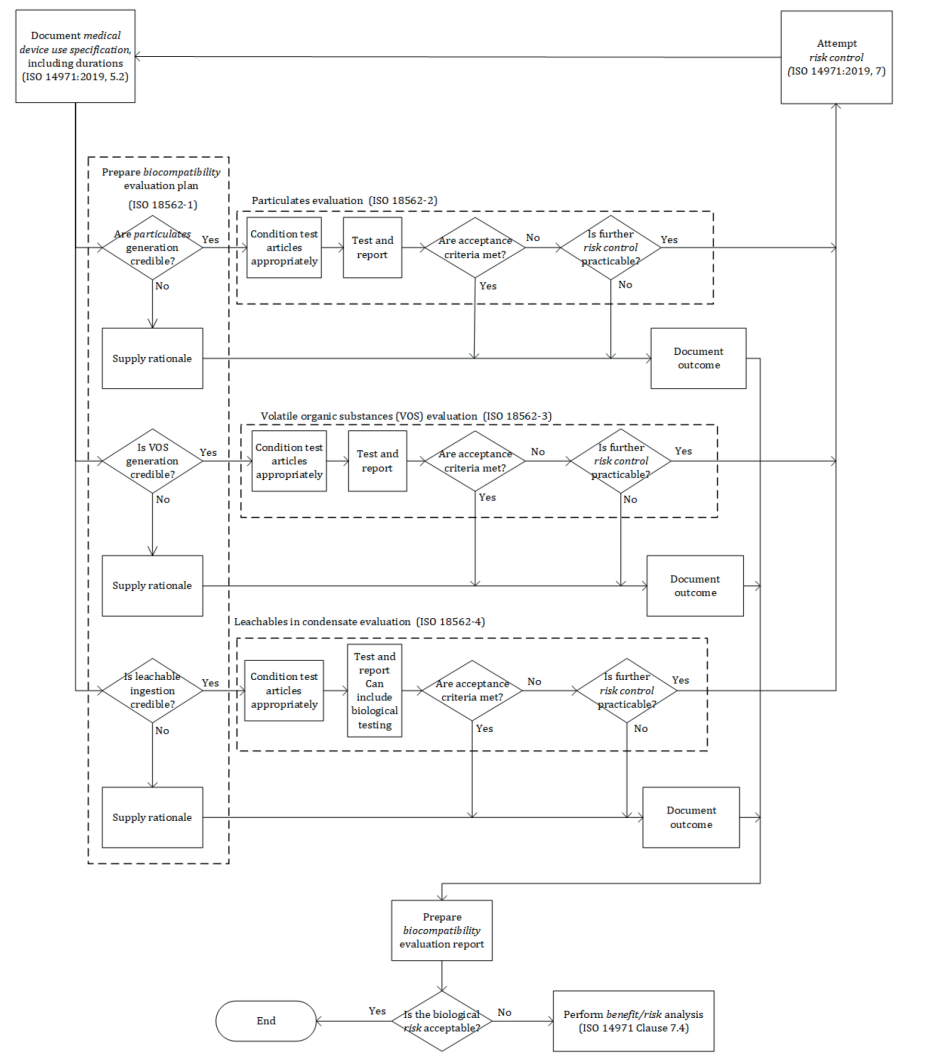
The diagram assessing the risk of use of a breathing medical device has been updated to a more comprehensive version including step by step the process to follow when addressing biocompatibility of a gas pathway medical device, see bellow new version as per 2024 standard.
Although the series do not address biocompatibility hazards associated with inorganic gases, the 2024 version of ISO 18562-1 mentioned that, when applicable and some authorities having jurisdiction require the manufacturer to evaluate the following:
— Ozone, for gas pathways in contact with active electromechanical or electrostatic parts in normal condition;
— CO, NOx and CO2, for gas pathways where inorganic gases are added, generated or concentrated;



")



